Patients ask me this almost every week, especially the ones who have spent some time on Google: “Shockwave or laser — which one’s going to help my whiplash?”
The honest answer is: it depends on what’s actually wrong. Whiplash isn’t one injury. It’s a category that covers everything from a mildly irritated cervical facet joint to a deep myofascial trigger-point cluster to a strained ligament that won’t settle down. Different problems respond to different inputs. Picking the right tool — or, more often, the right combination — is the part that actually moves the needle.
I’m Dr. Mike Kam, owner of Crash Care Clinics. We see whiplash every day, and we use both shockwave (extracorporeal shockwave therapy, ESWT) and Class IV laser (photobiomodulation) in our treatment rooms. This guide walks through how I think about choosing between them — what each one actually does at the tissue level, where the evidence is strong and where it isn’t, and how they fit alongside chiropractic adjustment and physical therapy, which are still the foundation of any auto-injury care plan.
The 30-second answer
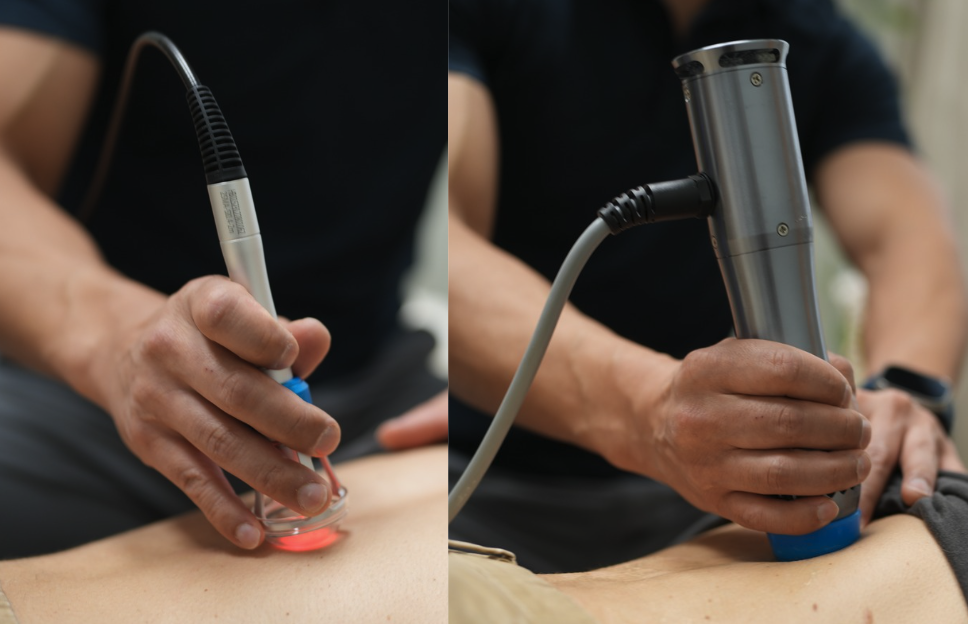
- Shockwave delivers focused mechanical pressure waves into deeper tissue. We use it for chronic myofascial trigger points, scar-tissue adhesions, and restricted areas that haven’t responded to manual care — typically once the acute inflammation has settled, often weeks 3-6 after the crash.
- Class IV laser delivers concentrated red and near-infrared light to drive cellular repair (photobiomodulation). We use it for acute inflammation, recent ligament/tendon strain, and symptom calming early in care — including the first few days after the collision.
- They aren’t competitors. Most of our whiplash plans use both — laser early to calm tissue, shockwave later to unstick what’s been stuck — alongside chiropractic adjustment and active rehab.
- All of this is covered by Oregon PIP if you have an auto policy. You don’t pay out of pocket for treatment.
First, what whiplash actually is
When someone asks “shockwave or laser for whiplash,” what they usually mean is “what fixes the pain in my neck after my crash.” That pain is doing several things at once.
The classic whiplash mechanism is rapid acceleration-deceleration of the head and neck — typically a rear-end impact. In the milliseconds during impact, the cervical spine forms an S-curve that hyperextends the lower levels and flexes the upper, which:
- Stretches the anterior longitudinal ligament and the anterior neck muscles (sternocleidomastoid, scalenes, longus colli)
- Compresses the cervical facet joints posteriorly — facet capsule injury is the most common identifiable pain generator in chronic whiplash
- Strains the paraspinal muscles posteriorly as they brace
- Often involves the upper trapezius, levator scapulae, and rhomboids as guarding patterns develop in the days after
Add in possible disc injury (the C5-C6 and C6-C7 levels take the most stress), vestibular involvement in higher-energy crashes, and autonomic dysregulation that explains the fatigue and brain fog patients report, and you get a picture that isn’t going to be solved by a single modality.
That’s the diagnostic backdrop. Now let’s look at the tools.
What shockwave (ESWT) actually does
Extracorporeal shockwave therapy delivers high-energy acoustic pressure waves into tissue. There are two flavors used clinically — focused shockwave, which concentrates energy at a specific depth, and radial pressure wave, which spreads energy more diffusely from the surface. Most chiropractic and PT offices use radial; some specialty clinics carry both. We use both at Crash Care.
What the wave actually does at the tissue level — based on the existing musculoskeletal literature — is:
- Triggers neovascularization (new small-vessel growth into hypoxic, scarred tissue)
- Disrupts calcific deposits and disorganized scar (best documented in calcific shoulder tendinopathy)
- Modulates nociceptor activity in chronic pain states — patients often describe a “reset” feeling after a session
- Stimulates fibroblast activity that supports proper collagen remodeling
Where the evidence is strongest — and where I have the most clinical confidence — is in chronic, well-localized, soft-tissue problems: lateral epicondylitis, chronic plantar fasciitis, greater trochanteric pain syndrome, calcific shoulder tendinopathy. Those are the indications backed by multiple randomized trials and meta-analyses.
For whiplash specifically, the high-quality randomized evidence is more limited. We use it because the myofascial trigger points and chronic muscle hypertonicity that show up weeks after a crash respond well in clinic — and that’s consistent with what the broader myofascial pain syndrome literature shows. I want to be straight about that: I’m extrapolating from related applications, not citing a definitive whiplash-specific trial.
When I reach for shockwave first:
- Patient is 3+ weeks post-crash, acute inflammation has settled, and there’s a ropey, palpable trigger point or band of tight tissue that hasn’t budged with manual therapy
- Persistent upper trapezius or levator scapulae tone that’s recreating headaches
- Suboccipital tightness driving cervicogenic headaches that aren’t fully responding to upper cervical adjustment
- Old scar tissue from a prior injury that’s now part of the picture
When I don’t:
- First week after the crash — too acute, will likely make things flare
- Active radiculopathy with numbness/tingling — needs different workup first
- Anyone on therapeutic anticoagulation — relative contraindication, requires medical clearance
- Over malignancy, near pacemakers, or in pregnant patients
What Class IV laser actually does
“Class IV” describes the power level of the device — anything above 500 milliwatts of output. The therapeutic lasers we use in clinic typically run somewhere between 10 and 25 watts at wavelengths in the 800-1064 nanometer range. (For context, Class IV is the same FDA classification as some surgical cutting lasers, but the therapeutic devices operate well below the heating threshold required to damage tissue.) The therapeutic mechanism is photobiomodulation, not thermal effect.
What that means at the cellular level:
- Photons in the red and near-infrared range are absorbed primarily by cytochrome c oxidase in mitochondria
- That absorption increases ATP production — more cellular energy available for repair
- It modulates reactive oxygen species in a way that reduces inflammatory signaling
- It increases nitric oxide release, which causes local vasodilation and improved microcirculation
- The net clinical effect is reduced inflammation, reduced pain, and accelerated tissue repair
Class IV laser was FDA-cleared in 2004 for pain reduction and increasing local microcirculation.
The whiplash-specific evidence is actually better than most patients realize. A 2013 randomized controlled trial out of Italy (Conforti & Fachinetti, Muscles, Ligaments and Tendons Journal) compared Class IV laser to conventional physical therapy in 135 patients with grade 1-2 whiplash:
- The laser group’s pain (VAS) dropped from 71 to 20 — the PT group dropped from 72 to 35
- The laser group returned to work an average of 54 days post-accident vs. 82 days for the PT-only group — a ~27% reduction in time off work, statistically significant
That’s a real, peer-reviewed RCT showing meaningful clinical benefit on the most relevant outcomes — pain and return to function — for the kind of whiplash that walks into our clinic every week.
When I reach for laser first:
- First few days to first three weeks after the crash, when tissue is acutely inflamed
- Recent ligament strain — the anterior cervical ligamentous injury that’s so common in rear-impact whiplash
- A patient who’s too sore for manual work and needs symptom-calming before they can tolerate adjustment or stretching
- Headaches in the first week after the crash, especially with photophobia or muscle-tension features
- Any patient where I want to drive tissue healing without adding mechanical input
When I don’t:
- Active malignancy in the treatment field (general contraindication for any modality stimulating tissue activity)
- Direct over the thyroid or eyes (we always use protective eyewear)
- Patients on photosensitizing medications without medical clearance — this is real; some antibiotics, chemotherapy agents, and tricyclic antidepressants increase photosensitivity
How to think about which one — the matrix
Most patients land in one of three buckets, and the modality choice follows the bucket.
Acute (week 1-2 post-crash): Laser does the heavy lifting. Tissue is inflamed and irritable. Mechanical input — including aggressive manual therapy, deep tissue, and shockwave — usually flares things. Laser calms inflammation, supports repair, and gets the patient tolerable enough for the rest of the plan.
Subacute (week 2-6): This is the transition. Acute inflammation is settling, but adhesions and trigger points are forming. Laser still has a role for residual inflammation. Adjustment + soft tissue + active rehab become the foundation. Shockwave starts to enter the conversation, especially for stubborn focal areas that aren’t releasing.
Chronic / persistent (week 6 onward): If pain is still present, it’s almost always being driven by adhesions, neuromuscular dysfunction, or unresolved tissue remodeling. Shockwave is most useful here. Laser has a smaller role, mostly for residual symptom control or flare-ups.
A real treatment plan from our clinic might look like: laser sessions in weeks 1-2 alongside gentle adjustment, transition to combined laser + shockwave on the trigger points in weeks 3-4, then shockwave + active rehab from week 5 onward, with laser available for symptom management.
Why we don’t pick — we combine
Most of our whiplash plans don’t choose between modalities. They use both, and they’re built on top of two things that matter more than either one:
- Chiropractic adjustment — directly addresses the joint dysfunction (especially the cervical facets) that drives most chronic whiplash pain. The ATP boost from laser and the tissue remodeling from shockwave both make the joint more responsive to adjustment, not less.
- Active rehab / physical therapy — restores motor control, strength, and proprioception that the crash disrupted. Whiplash patients who recover fastest are the ones who get out of “passive treatment only” mode by week 3-4 and start doing the work.
If a clinic is using shockwave or laser as the only thing they offer, that’s a red flag. These are tools to make the foundation work better, not substitutes for it. (For more on how to assess a clinic, see our first-visit guide.)
Honest evidence summary
I want to give you a clean read on where the evidence is for each:
Class IV laser for whiplash has at least one good-quality RCT (Conforti 2013) showing meaningful reductions in pain and time-off-work for grade 1-2 whiplash. Broader photobiomodulation evidence is strong for neck pain generally. My evidence confidence: moderate-to-high for symptomatic whiplash.
Shockwave for whiplash specifically has limited high-quality RCT data — the literature is dominated by tendinopathy and plantar fasciitis applications. Evidence for ESWT in myofascial pain syndrome (a 2025 scoping review in Life called for standardized protocols) and in chronic neck pain is encouraging but not yet definitive. My evidence confidence: moderate for the chronic, myofascial component of whiplash; lower as a primary first-line tool.
Both modalities are FDA-cleared, low-risk in appropriate patients, and a normal part of conservative auto-injury care. Neither is a miracle. Either one used in isolation will underperform compared to a coordinated plan that includes adjustment and active rehab.
Practical questions
How many sessions? A typical whiplash treatment course at our clinic runs 8-16 visits over 6-10 weeks, with modality selection adjusting as we move through phases. Some patients are out earlier; complex cases run longer. We re-evaluate every 4-6 visits.
What does it feel like? Laser feels warm — a noticeable but comfortable heat over the treatment area. Some patients feel a tingling or pulsing sensation. Shockwave is more intense — focused waves create a tapping or thumping sensation that can be tender over a trigger point. Most patients tolerate both well; we adjust intensity per session.
Will my insurance cover it? Yes, if you have Oregon auto insurance. Personal Injury Protection (PIP) — minimum $15,000 over a 2-year window, no fault required — covers chiropractic, PT, and modality-based care after an auto injury. We bill PIP directly. Most of our auto-injury patients pay nothing out of pocket. Health insurance also covers these modalities for many policies, but PIP is faster and easier when there’s been a crash. See our Oregon PIP guide for the full breakdown.
Should I pick a clinic that has both? It helps. A clinic with only one of these modalities will sometimes use the wrong tool for the job — not out of bad intent, but because it’s the only tool they have. A clinic with both can match the modality to the phase of healing.
Is shockwave or laser better for whiplash? Neither is universally better — they treat different problems. Class IV laser is generally a better fit during the first few weeks after a crash (acute inflammation, recent ligament strain). Shockwave is a better fit for chronic myofascial trigger points and adhesions that show up weeks later. Most whiplash treatment plans use both, sequenced by stage of healing.
Does Class IV laser actually have evidence for whiplash? Yes. A 2013 randomized controlled trial of 135 grade 1-2 whiplash patients (Conforti & Fachinetti, Muscles, Ligaments and Tendons Journal) showed Class IV laser produced significantly greater pain reduction (VAS 71→20 vs 72→35) and a 27% faster return to work compared to conventional physical therapy alone.
Is shockwave therapy safe after a car accident? In the right patient and at the right time, yes. We don’t typically use shockwave in the first week or two after a crash because the tissue is too acutely inflamed. Once the acute phase has settled — usually around week 3 onward — shockwave is well-tolerated for most patients. It’s not appropriate for anyone on therapeutic anticoagulants, with active malignancy in the treatment area, with a pacemaker in the field, or who is pregnant.
How many laser or shockwave sessions will I need? Most whiplash treatment plans at our clinic include 8-16 total visits over 6-10 weeks, with modality selection shifting as care progresses. Mild cases may resolve in fewer; complex cases need more. We re-evaluate progress every 4-6 visits and adjust the plan based on what’s actually happening.
Does Oregon PIP pay for shockwave and laser therapy? Yes. Oregon PIP (ORS 742.524) covers medically necessary chiropractic, physical therapy, and modality-based treatment for auto injuries — including shockwave and Class IV laser when indicated. Minimum $15,000 in coverage with a 2-year window, no fault required. We bill PIP directly so there’s no out-of-pocket cost at the front desk.
Can I just pick one? You can, and some patients do — for budget reasons in a non-PIP situation, or because of personal preference. But in our clinic, the patients who recover fastest are the ones using both modalities matched to the right stage of healing, on top of a foundation of chiropractic adjustment and active rehab. The modalities make the foundation work better. None of them substitute for it.
- Conforti M, Fachinetti GP. High power laser therapy treatment compared to simple segmental physical rehabilitation in whiplash injuries. Muscles, Ligaments and Tendons Journal, 2013;3(2):106–111.
- The State of Extracorporeal Shockwave Therapy for Myofascial Pain Syndrome — A Scoping Review and Call for Standardized Protocols. Life, 2025.
- Extracorporeal Shock Wave Therapy for the Treatment of Musculoskeletal Pain: A Narrative Review. Healthcare, 2023.
- Oregon Revised Statutes 742.524 — Personal Injury Protection benefits


Leave a Reply